Blank Annual Physical Examination PDF Form
Documents PDF
Blank Annual Physical Examination PDF Form
The Annual Physical Examination form serves as a comprehensive tool designed to facilitate a thorough assessment of an individual's health status. It is essential for patients to complete all sections of the form prior to their medical appointment to minimize the need for return visits. The first part of the form requires personal information, including the patient's name, date of birth, and medical history, as well as details about current medications and any allergies. This section also covers immunization records, tuberculosis screening, and a list of any significant health conditions. The second part of the form focuses on the general physical examination, where vital signs such as blood pressure, pulse, and temperature are recorded. A systematic evaluation of various body systems follows, allowing healthcare providers to note any normal findings or areas requiring further attention. Additional comments can include recommendations for health maintenance, dietary instructions, and any limitations on activities. By gathering this information, the Annual Physical Examination form not only streamlines the examination process but also ensures that healthcare providers have a clear understanding of each patient's unique health needs.
Once you have gathered all necessary information, you can begin filling out the Annual Physical Examination form. Make sure to complete all sections to avoid any delays or return visits.
Here are seven misconceptions about the Annual Physical Examination form:
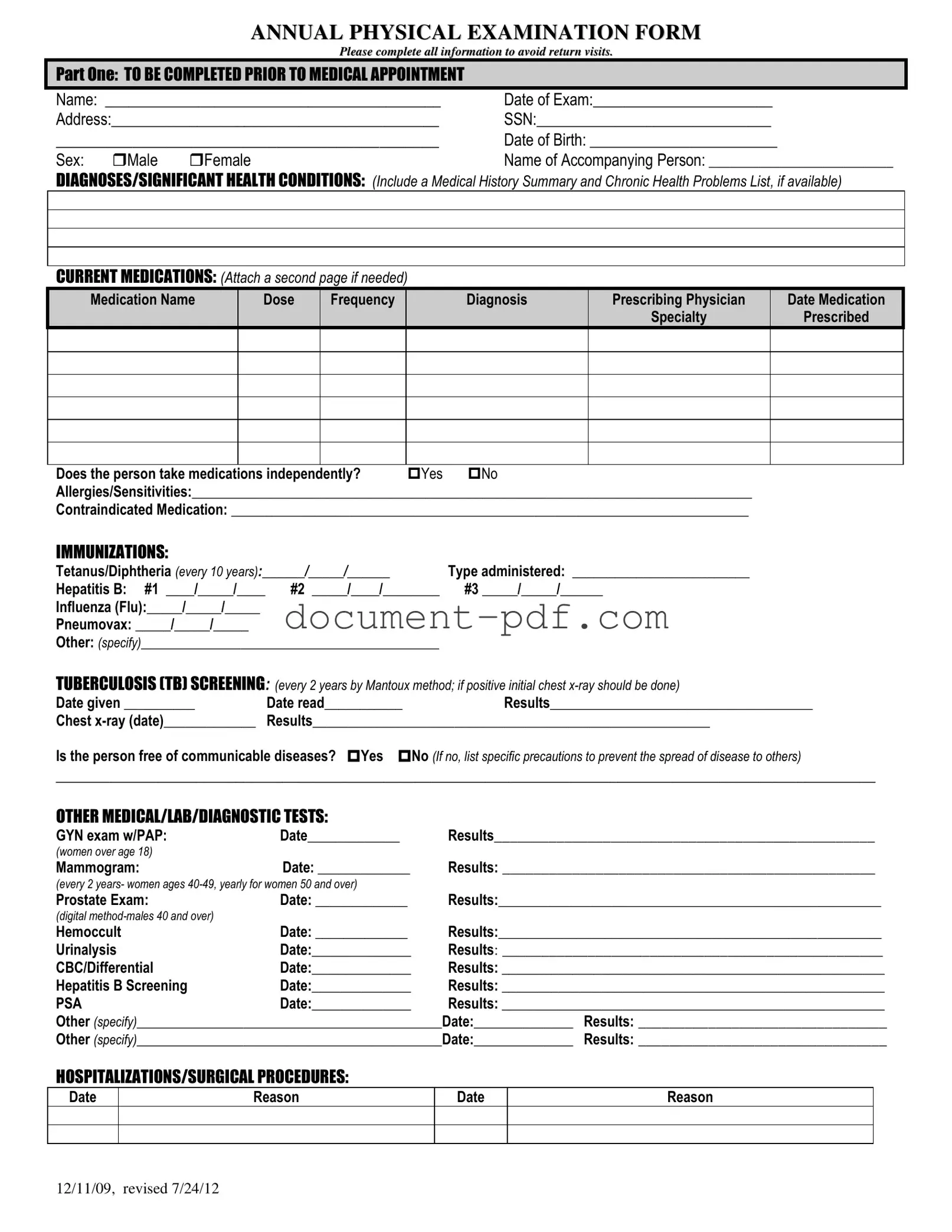
ANNUAL PHYSICAL EXAMINATION FORM
Please complete all information to avoid return visits.
PART ONE: TO BE COMPLETED PRIOR TO MEDICAL APPOINTMENT
Name: ___________________________________________ |
Date of Exam:_______________________ |
Address:__________________________________________ |
SSN:______________________________ |
_____________________________________________ |
Date of Birth: ________________________ |
||
Sex: |
Male |
Female |
Name of Accompanying Person: __________________________ |
DIAGNOSES/SIGNIFICANT HEALTH CONDITIONS: (Include a Medical History Summary and Chronic Health Problems List, if available)
CURRENT MEDICATIONS: (Attach a second page if needed)
Medication Name |
Dose |
Frequency |
Diagnosis |
Prescribing Physician |
Date Medication |
|
|
|
|
Specialty |
Prescribed |
Does the person take medications independently? |
Yes |
No |
Allergies/Sensitivities:_______________________________________________________________________________ |
||
Contraindicated Medication: _________________________________________________________________________
IMMUNIZATIONS:
Tetanus/Diphtheria (every 10 years):______/_____/______ |
Type administered: _________________________ |
|
Hepatitis B: #1 ____/_____/____ |
#2 _____/____/________ |
#3 _____/_____/______ |
Influenza (Flu):_____/_____/_____ |
|
|
Pneumovax: _____/_____/_____ |
|
|
Other: (specify)__________________________________________ |
|
|
TUBERCULOSIS (TB) SCREENING: (every 2 years by Mantoux method; if positive initial chest |
||
Date given __________ |
Date read___________ |
Results_____________________________________ |
Chest |
Results________________________________________________________ |
|
Is the person free of communicable diseases? Yes No (If no, list specific precautions to prevent the spread of disease to others)
_________________________________________________________________________________________________________
OTHER MEDICAL/LAB/DIAGNOSTIC TESTS:
GYN exam w/PAP: |
Date_____________ |
Results_________________________________________________ |
(women over age 18) |
|
|
Mammogram: |
Date: _____________ |
Results: ________________________________________________ |
(every 2 years- women ages
Prostate Exam: |
Date: _____________ |
Results:______________________________________________________ |
|
(digital |
|
|
|
Hemoccult |
Date: _____________ |
Results:______________________________________________________ |
|
Urinalysis |
Date:______________ |
Results: _________________________________________________ |
|
CBC/Differential |
Date:______________ |
Results: ______________________________________________________ |
|
Hepatitis B Screening |
Date:______________ |
Results: ______________________________________________________ |
|
PSA |
Date:______________ |
Results: ______________________________________________________ |
|
Other (specify)___________________________________________Date:______________ |
Results: ________________________________ |
||
Other (specify)___________________________________________Date:______________ |
Results: ________________________________ |
||
HOSPITALIZATIONS/SURGICAL PROCEDURES:
Date
Reason
Date
Reason
12/11/09, revised 7/24/12

PART TWO: GENERAL PHYSICAL EXAMINATION
|
|
|
|
|
Please complete all information to avoid return visits. |
|
|
|
|
|
Blood Pressure:______ /_______ Pulse:_________ |
Respirations:_________ Temp:_________ Height:_________ |
Weight:_________ |
||||
|
|
EVALUATION OF SYSTEMS |
|
|
|
|
||
|
|
|
|
|
|
|
||
|
|
System Name |
|
Normal Findings? |
Comments/Description |
|
||
|
|
Eyes |
|
Yes |
No |
|
|
|
|
|
Ears |
|
Yes |
No |
|
|
|
|
|
Nose |
|
Yes |
No |
|
|
|
|
|
Mouth/Throat |
|
Yes |
No |
|
|
|
|
|
Head/Face/Neck |
|
Yes |
No |
|
|
|
|
|
Breasts |
|
Yes |
No |
|
|
|
|
|
Lungs |
|
Yes |
No |
|
|
|
|
|
Cardiovascular |
|
Yes |
No |
|
|
|
|
|
Extremities |
|
Yes |
No |
|
|
|
|
|
Abdomen |
|
Yes |
No |
|
|
|
|
|
Gastrointestinal |
|
Yes |
No |
|
|
|
|
|
Musculoskeletal |
|
Yes |
No |
|
|
|
|
|
Integumentary |
|
Yes |
No |
|
|
|
|
|
Renal/Urinary |
|
Yes |
No |
|
|
|
|
|
Reproductive |
|
Yes |
No |
|
|
|
|
|
Lymphatic |
|
Yes |
No |
|
|
|
|
|
Endocrine |
|
Yes |
No |
|
|
|
|
|
Nervous System |
|
Yes |
No |
|
|
|
|
|
VISION SCREENING |
|
Yes |
No |
Is further evaluation recommended by specialist? |
Yes |
No |
|
|
HEARING SCREENING |
|
Yes |
No |
Is further evaluation recommended by specialist? |
Yes |
No |
|
|
ADDITIONAL COMMENTS: |
|
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
Medical history summary reviewed? |
Yes |
No |
|
|
||
Medication added, changed, or deleted: (from this appointment)__________________________________________________________
Special medication considerations or side effects: ________________________________________________________________
Recommendations for health maintenance: (include need for lab work at regular intervals, treatments, therapies, exercise, hygiene, weight control, etc.)
___________________________________________________________________________________________________________
Recommendations for manual breast exam or manual testicular exam: (include who will perform and frequency)____________________
___________________________________________________________________________________________________________
Recommended diet and special instructions: ____________________________________________________________________
Information pertinent to diagnosis and treatment in case of emergency:
___________________________________________________________________________________________________________
Limitations or restrictions for activities (including work day, lifting, standing, and bending): No Yes (specify)
___________________________________________________________________________________________________________ |
|||
Does this person use adaptive equipment? |
No |
Yes (specify):________________________________________________ |
|
Change in health status from previous year? No |
Yes (specify):_________________________________________________ |
||
This individual is recommended for ICF/ID level of care? (see attached explanation) Yes |
No |
||
Specialty consults recommended? No |
Yes (specify):_________________________________________________________ |
||
Seizure Disorder present? No Yes (specify type):__________________________________ Date of Last Seizure: ______________ |
|||
________________________________ |
_______________________________ |
_________________ |
|
Name of Physician (please print) |
Physician’s Signature |
|
Date |
Physician Address: _____________________________________________ |
Physician Phone Number: ____________________________ |
||
12/11/09, revised 7/24/12
Filling out the Annual Physical Examination form accurately is crucial for ensuring a smooth and efficient medical appointment. Here are five key takeaways to keep in mind:
By keeping these takeaways in mind, you can make the most out of your annual physical examination and ensure that your healthcare provider has all the necessary information to assist you effectively.
Profits or Loss From Business - Reporting on Schedule C helps fulfill legal obligations while allowing for potential deductions.
When preparing for unforeseen circumstances, it’s important to have a plan in place, and the Texas Power of Attorney form serves as a crucial tool in that regard. By using this legal document, an individual can designate someone to make essential decisions on their behalf, covering areas such as financial obligations and health care. If you're looking for resources to create this document, you can find a useful template at texasformsonline.com/free-power-of-attorney-template, ensuring that your preferences are respected even when you are unable to communicate them yourself.
Western Union Form - Make your international transfers simple and transparent.
When filling out the Annual Physical Examination form, it is important to ensure accuracy and completeness. Here are seven essential tips to keep in mind:
Following these guidelines will help ensure that your Annual Physical Examination goes smoothly and that your healthcare provider has all the necessary information to assist you effectively.
The Health History Questionnaire serves a similar purpose to the Annual Physical Examination form by collecting detailed information about an individual's medical background. It typically includes sections for personal information, medical history, current medications, allergies, and family medical history. Both documents aim to ensure that healthcare providers have a comprehensive understanding of a patient's health status before conducting an examination or treatment.
The Patient Intake Form is another document that shares similarities with the Annual Physical Examination form. This form is often used in medical offices to gather essential information from new patients. It includes sections for personal details, insurance information, medical history, and current medications. Like the Annual Physical Examination form, it seeks to streamline the process of obtaining relevant health information prior to a medical appointment.
The Medication Reconciliation Form is closely related to the Annual Physical Examination form, particularly in its focus on current medications. This document is used to compare a patient's medication list against their current prescriptions to identify any discrepancies or potential interactions. Both forms emphasize the importance of accurate medication information for safe and effective healthcare delivery.
The Immunization Record is another document that parallels the Annual Physical Examination form. It tracks a patient's vaccination history, including dates and types of immunizations received. Both documents play a crucial role in ensuring that individuals are up to date on necessary vaccinations, which is vital for preventive health measures.
The Lab Test Requisition Form is similar to the Annual Physical Examination form in that it specifies tests that need to be performed based on a patient's health status. This form typically includes patient information, the specific tests ordered, and any relevant clinical information. Both documents are essential for guiding healthcare providers in assessing a patient's health through diagnostic testing.
The Consent for Treatment Form is another document that serves a similar function to the Annual Physical Examination form. It ensures that patients understand and agree to the procedures and examinations they will undergo. Both documents are critical for establishing clear communication between patients and healthcare providers, fostering informed consent.
The Medical Release Form is akin to the Annual Physical Examination form in that it allows healthcare providers to share a patient’s medical information with other parties, such as specialists or insurance companies. Both documents facilitate the flow of essential health information, which is vital for coordinated care and treatment planning.
For individuals looking to prepare their legal documents, the Last Will and Testament serves a similar purpose to the Annual Physical Examination form by ensuring that important aspects of one’s life are documented comprehensively. It emphasizes the significance of clear instruction regarding asset distribution after death, providing assurance that one’s wishes will be respected. For more information on how to create your Last Will and Testament, you can visit pdfdocshub.com/.
The Advance Directive Form shares similarities with the Annual Physical Examination form by addressing a patient's preferences for medical treatment in the event they are unable to communicate their wishes. Both documents focus on the patient's health and well-being, ensuring that their values and preferences are respected in medical decision-making.
The Follow-Up Appointment Form is another document that is similar to the Annual Physical Examination form. It is used to schedule and confirm subsequent visits based on the findings from the initial examination. Both documents aim to enhance continuity of care by ensuring that patients receive appropriate follow-up for any identified health concerns.
Finally, the Chronic Disease Management Plan is closely related to the Annual Physical Examination form. This document outlines a strategy for managing ongoing health conditions, including medications, lifestyle changes, and regular monitoring. Both documents emphasize proactive health management to improve patient outcomes and quality of life.