Blank DD 2870 PDF Form
Documents PDF
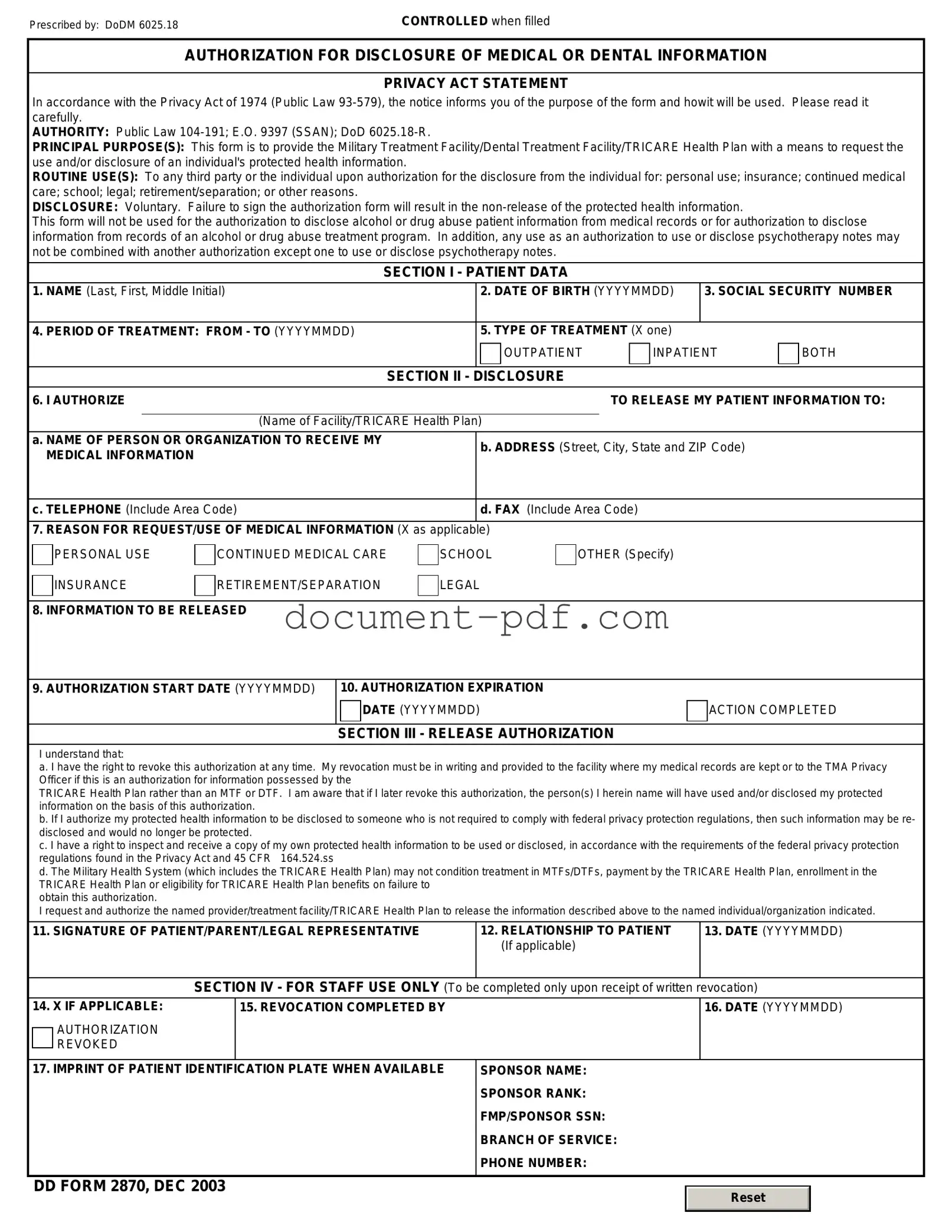
Blank DD 2870 PDF Form
The DD 2870 form plays an important role for individuals seeking to access their military medical records. This form is specifically designed for service members, veterans, and eligible family members to authorize the release of their medical information. By completing the DD 2870, individuals can ensure that their health records are shared with the appropriate healthcare providers or organizations, facilitating continuity of care. It also allows for the transfer of medical information when transitioning from military to civilian healthcare systems. Understanding the requirements and process for filling out this form is crucial for anyone needing to manage their health records effectively. Additionally, knowing how to submit the form and what to expect after submission can help alleviate any concerns regarding privacy and the handling of sensitive information. Overall, the DD 2870 is a vital tool for maintaining access to essential medical services.
Filling out the DD 2870 form is an important step for individuals seeking certain benefits or services. After completing the form, it will need to be submitted to the appropriate authority for processing. Below are the steps to guide you through the completion of the form.
The DD 2870 form, also known as the "Authorization for Disclosure of Medical or Dental Information," is often misunderstood. Here are nine common misconceptions about this form:
Understanding these misconceptions can help individuals navigate the process of using the DD 2870 form more effectively.
Prescribed by: DoDM 6025.18 |
CONTROLLED when filled |
AUTHORIZATION FOR DISCLOSURE OF MEDICAL OR DENTAL INFORMATION
PRIVACY ACT STATEMENT
In accordance with the Privacy Act of 1974 (Public Law
AUTHORITY: Public Law
PRINCIPAL PURPOSE(S): This form is to provide the Military Treatment Facility/Dental Treatment Facility/TRICARE Health Plan with a means to request the use and/or disclosure of an individual's protected health information.
ROUTINE USE(S): To any third party or the individual upon authorization for the disclosure from the individual for: personal use; insurance; continued medical care; school; legal; retirement/separation; or other reasons.
DISCLOSURE: Voluntary. Failure to sign the authorization form will result in the
This form will not be used for the authorization to disclose alcohol or drug abuse patient information from medical records or for authorization to disclose information from records of an alcohol or drug abuse treatment program. In addition, any use as an authorization to use or disclose psychotherapy notes may not be combined with another authorization except one to use or disclose psychotherapy notes.
SECTION I - PATIENT DATA
1. NAME (Last, First, Middle Initial) |
|
2. DATE OF BIRTH (YYYYMMDD) |
3. SOCIAL SECURITY NUMBER |
|||
|
|
|
|
|
|
|
4. PERIOD OF TREATMENT: FROM - TO (YYYYMMDD) |
|
5. TYPE OF TREATMENT (X one) |
|
|
||
|
|
|
OUTPATIENT |
INPATIENT |
BOTH |
|
|
|
|
|
|
|
|
|
|
SECTION II - |
DISCLOSURE |
|
|
|
6. I AUTHORIZE |
|
|
TO RELEASE MY PATIENT INFORMATION TO: |
|||
|
|
|
|
|
||
|
(Name of Facility/TRICARE Health Plan) |
|
|
|
||
a. NAME OF PERSON OR ORGANIZATION TO RECEIVE MY |
|
b. ADDRESS (Street, City, State and ZIP Code) |
|
|||
MEDICAL INFORMATION |
|
|
||||
|
|
|
|
|
||
|
|
|
|
|
||
c. TELEPHONE (Include Area Code) |
|
d. FAX (Include Area Code) |
|
|
||
|
|
|
|
|
||
7. REASON FOR REQUEST/USE OF MEDICAL INFORMATION (X as applicable) |
|
|
|
|
||
PERSONAL USE
INSURANCE
CONTINUED MEDICAL CARE
RETIREMENT/SEPARATION
SCHOOL
LEGAL
OTHER (Specify)
8. INFORMATION TO BE RELEASED
9. AUTHORIZATION START DATE (YYYYMMDD)
10. AUTHORIZATION EXPIRATION
DATE (YYYYMMDD)
SECTION III - RELEASE AUTHORIZATION
ACTION COMPLETED
I understand that:
a. I have the right to revoke this authorization at any time. My revocation must be in writing and provided to the facility where my medical records are kept or to the TMA Privacy Officer if this is an authorization for information possessed by the
TRICARE Health Plan rather than an MTF or DTF. I am aware that if I later revoke this authorization, the person(s) I herein name will have used and/or disclosed my protected information on the basis of this authorization.
b. If I authorize my protected health information to be disclosed to someone who is not required to comply with federal privacy protection regulations, then such information may be re- disclosed and would no longer be protected.
c. I have a right to inspect and receive a copy of my own protected health information to be used or disclosed, in accordance with the requirements of the federal privacy protection regulations found in the Privacy Act and 45 CFR 164.524.ss
d. The Military Health System (which includes the TRICARE Health Plan) may not condition treatment in MTFs/DTFs, payment by the TRICARE Health Plan, enrollment in the TRICARE Health Plan or eligibility for TRICARE Health Plan benefits on failure to
obtain this authorization.
I request and authorize the named provider/treatment facility/TRICARE Health Plan to release the information described above to the named individual/organization indicated.
11. SIGNATURE OF PATIENT/PARENT/LEGAL REPRESENTATIVE |
12. RELATIONSHIP TO PATIENT |
13. DATE (YYYYMMDD) |
|
(If applicable) |
|
|
|
|
SECTION IV - FOR STAFF USE ONLY (To be |
completed only upon receipt of written revocation) |
|
14. X IF APPLICABLE:
AUTHORIZATION REVOKED
15. REVOCATION COMPLETED BY
16.DATE (YYYYMMDD)
17. IMPRINT OF PATIENT IDENTIFICATION PLATE WHEN AVAILABLE |
SPONSOR NAME: |
||
|
SPONSOR RANK: |
||
|
FMP/SPONSOR SSN: |
||
|
BRANCH OF SERVICE: |
||
|
PHONE NUMBER: |
||
|
|
|
|
DD FORM 2870, DEC 2003 |
|
|
|
|
Reset |
|
|
|
|
|
|
|
|
|
|
The DD 2870 form is essential for individuals seeking to access their medical records or request information related to their health care. Here are nine key takeaways regarding its use:
California Corrective Deed - The Scrivener's Affidavit helps to eliminate ambiguities regarding the creation of the related legal document.
To facilitate a smooth real estate transaction, it is highly recommended to utilize a comprehensive Real Estate Purchase Agreement, such as the one available at texasformsonline.com/free-real-estate-purchase-agreement-template/, which can help both buyers and sellers clearly define their respective rights and obligations, thus minimizing misunderstandings and disputes.
Advance Salary Format - Request funds to pay for essential supplies ahead of time.
Column Chart - Concise Communication: This format forces you to communicate your thoughts concisely.
When filling out the DD 2870 form, it is essential to follow specific guidelines to ensure accuracy and compliance. Below is a list of things you should and shouldn't do.
Following these guidelines will help ensure that your DD 2870 form is completed correctly and processed efficiently.
The DD Form 2870, also known as the Authorization for Disclosure of Medical or Dental Information, is similar to the HIPAA Authorization form. Both documents allow individuals to grant permission for healthcare providers to share their medical information with specific third parties. This ensures that personal health data can be communicated appropriately while maintaining compliance with privacy regulations. The key difference lies in the scope; the DD Form 2870 is specifically tailored for military personnel and veterans, while the HIPAA Authorization is applicable to the general population.
The New York Trailer Bill of Sale is a legal document used to transfer ownership of a trailer from one person to another within the state of New York. This form outlines essential details such as the trailer's specifications, the sale price, and the identities of both the buyer and seller. Properly completing this document ensures a smooth transfer and helps avoid potential disputes in the future. For more information on how to obtain this form, visit New York PDF Docs.
Another document that resembles the DD Form 2870 is the Patient Authorization for Release of Information. This form is often used in various healthcare settings to allow patients to authorize the release of their medical records. Like the DD Form 2870, it requires the patient to specify who can access their information and for what purpose. Both forms aim to protect patient confidentiality while enabling necessary communication between medical professionals and other parties.
The Consent for Treatment form shares similarities with the DD Form 2870 in that both require patient consent before medical services can be provided. While the DD Form 2870 focuses on the disclosure of information, the Consent for Treatment form emphasizes the patient's agreement to receive care. Both forms are essential in ensuring that patients are informed and that their rights are respected within the healthcare system.
The Medical Records Release form also aligns with the DD Form 2870. This document allows patients to authorize the release of their medical records to designated individuals or organizations. Like the DD Form 2870, it emphasizes patient control over who has access to their sensitive health information. The primary distinction is that the Medical Records Release form is often used in civilian healthcare settings, whereas the DD Form 2870 is specific to military contexts.
The Authorization for Use or Disclosure of Protected Health Information (PHI) is another document similar to the DD Form 2870. This form is commonly used to allow healthcare providers to share PHI with third parties. Both documents serve to protect patient privacy while facilitating the necessary exchange of information. The PHI authorization form is broader in scope, applicable to various healthcare scenarios, while the DD Form 2870 is focused on military and veteran healthcare needs.
The Release of Information Consent form is also comparable to the DD Form 2870. This form enables individuals to give consent for their medical records to be shared with specific entities. Both forms are designed to ensure that individuals are aware of and agree to the sharing of their health information. The Release of Information Consent form is frequently used in various healthcare environments, while the DD Form 2870 is specifically for military-related healthcare disclosures.
The Authorization for Release of Medical Records is another document akin to the DD Form 2870. This form allows patients to authorize healthcare providers to release their medical records to specified individuals or organizations. Both documents require clear consent from the patient and serve the purpose of facilitating communication while safeguarding patient privacy. However, the Authorization for Release of Medical Records is typically used in civilian healthcare, whereas the DD Form 2870 is intended for military personnel.
Lastly, the General Release of Information form has similarities with the DD Form 2870. This document allows individuals to grant permission for the release of various types of information, including medical records. Both forms emphasize the importance of informed consent and the protection of personal information. The General Release of Information form can be used in a variety of contexts, while the DD Form 2870 is specifically designed for military-related healthcare situations.