Blank Medication Administration Record Sheet PDF Form
Documents PDF
Blank Medication Administration Record Sheet PDF Form
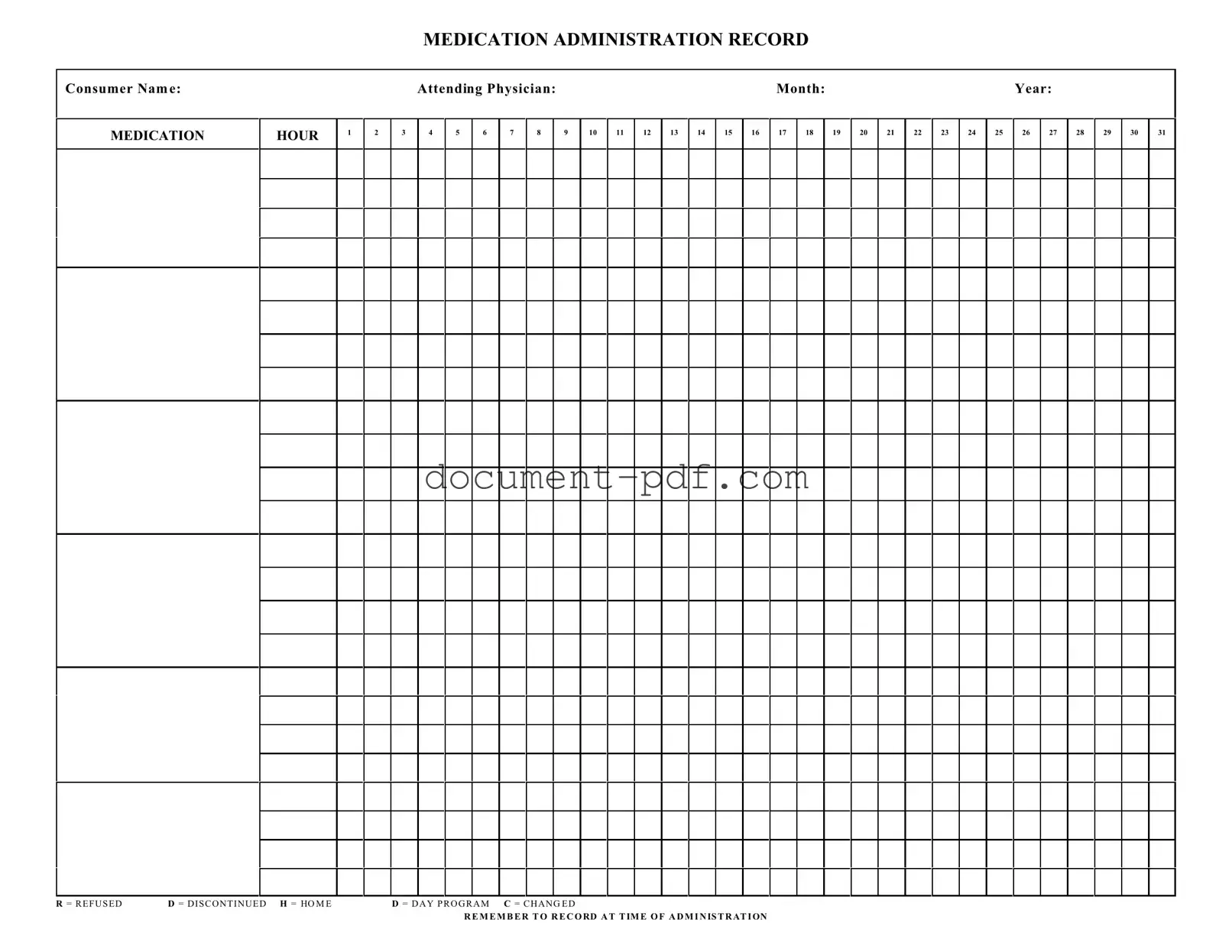
The Medication Administration Record Sheet is a crucial tool in healthcare settings, ensuring that patients receive their medications accurately and on time. This form captures essential details, including the consumer's name, the attending physician, and the month and year of administration. It provides a structured way to document medication schedules, allowing healthcare providers to track dosages administered at specific hours throughout the day. Each hour of the day is represented, with designated spaces to record whether a dose was given, refused, or discontinued. Additionally, the form includes specific codes for various situations, such as “H” for home and “D” for day program, which helps in maintaining clarity about the patient's medication regimen. It is vital for caregivers to remember to record the administration time, as this information is critical for ongoing patient care and compliance with medical protocols. By systematically organizing this information, the Medication Administration Record Sheet enhances communication among healthcare providers and supports patient safety.
Completing the Medication Administration Record Sheet is an essential step in ensuring proper medication management. This form allows for clear documentation of medication administration, helping to maintain accurate health records. Follow these steps to fill out the form correctly.
By following these steps, you can ensure that the Medication Administration Record Sheet is filled out accurately and completely, facilitating effective communication among healthcare providers and caregivers.
Misconceptions about the Medication Administration Record Sheet form can lead to confusion and errors in medication management. Here are four common misunderstandings:
MEDICATION ADMINISTRATION RECORD
Consumer Nam e:
MEDICATION
HOUR
1
2
|
Attending Physician: |
|
|
|
|
|
|
|
|
Month: |
|
|
|
|
|
|
|
Year: |
|
|
|
|
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
3 |
4 |
5 |
6 |
7 |
8 |
|
9 |
10 |
11 |
12 |
13 |
14 |
15 |
16 |
17 |
18 |
|
19 |
20 |
21 |
22 |
23 |
24 |
25 |
26 |
27 |
28 |
29 |
30 |
31 |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
R = R E F U S E D |
D = D I S C O N T I N U E D H = HO M E |
D = D A Y P R O G R A M C = C H A N G E D |
R E M E M B E R T O R E C O RD A T T IM E O F A D M I N IS T R AT I ON
Filling out and using the Medication Administration Record Sheet (MARS) is crucial for ensuring that medication is administered safely and effectively. Here are some key takeaways to keep in mind:
By following these guidelines, you can help ensure that the medication administration process is smooth and effective, ultimately leading to better health outcomes for consumers.
Employer's Quarterly Federal Tax Return - Form 941 is used to communicate changes in employment tax circumstances to the IRS.
Obtaining a Texas RV Bill of Sale is a vital step when purchasing or selling a recreational vehicle, as it ensures both parties are protected and the transaction is documented properly. For those looking for a detailed and straightforward template to assist in this process, you can find one at texasformsonline.com/free-rv-bill-of-sale-template/, which simplifies the creation of this important document.
Who Needs a 1099 Nec - Only the official printed version of Copy A can be filed with the IRS.
When filling out the Medication Administration Record Sheet, it is essential to follow certain guidelines to ensure accuracy and compliance. Below is a list of actions to take and avoid.
The Medication Administration Record (MAR) is similar to the Patient Medication List. Both documents track the medications a patient is prescribed. The Patient Medication List provides a comprehensive overview of all medications, including dosages and schedules. In contrast, the MAR focuses specifically on the administration of those medications, documenting when each dose is given or if it was refused. This ensures that healthcare providers have a clear record of what has been administered to the patient.
Another document similar to the MAR is the Medication Reconciliation Form. This form is used to compare a patient's current medications with those they have been prescribed or have been taking. While the MAR records administration, the Medication Reconciliation Form aims to identify discrepancies and ensure patient safety. Both documents are essential for maintaining accurate medication records and preventing errors in treatment.
The Nursing Medication Administration Record is also akin to the MAR. This record is specifically used by nursing staff to document the administration of medications to patients. It includes similar fields for recording the time and dosage of medications given. Both documents serve to ensure that medications are administered according to the prescribed schedule and that any issues, such as refusals, are noted.
The Prescription Log shares similarities with the MAR as well. The Prescription Log tracks the medications that have been prescribed to a patient, including details about the prescribing physician and the pharmacy. While the MAR focuses on administration, the Prescription Log provides a broader context of the patient's medication history. Both documents are crucial for ensuring proper medication management.
In the realm of medical documentation, having a reliable source for templates can greatly facilitate the process of maintaining accurate and efficient records. For those seeking a well-structured Bill of Sale form, the Texas PDF Templates provides an excellent resource to help streamline this essential aspect of property ownership transfer while ensuring all necessary details are captured effectively.
The Treatment Administration Record (TAR) is another related document. The TAR is used to record not only medications but also other treatments provided to a patient, such as injections or physical therapy. Like the MAR, it documents the time and details of each treatment. This ensures that all aspects of a patient's care are tracked and managed effectively.
The Controlled Substance Log is similar to the MAR in that it tracks the administration of controlled medications. This log is specifically designed to ensure that controlled substances are accounted for properly. It includes details about the medication, dosage, and administration time, much like the MAR. Both documents are critical for compliance with regulations surrounding medication management.
The Incident Report Form can also be compared to the MAR. While the MAR records routine administration of medications, the Incident Report Form is used to document any adverse events or medication errors. Both forms are vital for ensuring patient safety and improving healthcare practices. They help identify areas for improvement in medication administration processes.
The Daily Progress Notes are another document that shares similarities with the MAR. These notes provide a daily record of a patient's condition and any treatments administered, including medications. While the MAR focuses specifically on medication administration, the Daily Progress Notes offer a broader view of the patient's overall care. Both documents are important for maintaining accurate records and ensuring continuity of care.
Lastly, the Care Plan is similar to the MAR in that it outlines the overall treatment strategy for a patient, including medication management. The Care Plan details the goals and interventions for a patient's care, while the MAR provides a specific record of medication administration. Both documents work together to ensure that a patient's needs are met effectively and that their treatment is coordinated among healthcare providers.